In either case, the doctor will first use a smaller needle to numb up the skin around the biopsy site to help minimize any discomfort or pain. For most biopsy procedures, you will usually be awake, with the exception of a surgical biopsy. Procedures also vary in the digital imaging technology used to guide the doctor to the area from which the sample is to be taken.
Your doctor chooses the type of breast biopsy that will deliver the most accurate and useful results based on conditions detected in previous diagnostic examinations, as shown in the table.
Choosing a Breast Biopsy Type
| Condition | Breast biopsy type | Description |
| Mass detected via mammogram or ultrasound | Ultrasound-guided core needle biopsy. | A thin, hollow needle is injected into the mass under the guidance of ultrasound, to collect one or more samples. |
| Abnormal calcifications appearing as white spots on mammogram but that can't be felt | Stereotactic biopsy (you can have this procedure done in sitting position or lying face down, depending on the type of machine). | Breast tissue samples of the abnormal area are taken under the guidance of mammogram images. |
| Lesion (area of abnormal tissue) or abnormal breast finding only seen on MRI | MRI-guided core needle biopsy. | Breast tissue samples of the abnormal area are taken under the guidance of a breast MRI. |
| Suspicious lump in breast or under arm that can be felt during a clinical breast exam | Fine needle aspiration biopsy (ultrasound-guided core biopsy is often preferred because more tissue is collected to get a definitive diagnosis). | A very fine needle is attached to a syringe and a small amount of tissue and sometimes fluid is withdrawn from the lump. Useful for distinguishing between a fluid-filled cyst and a solid mass. |
| Blisters or ulcerated skin on the breast | Skin-punch biopsy. | A circular tool is used to remove a small section of the skin and deeper layers of the breast tissue. |
| Breast mass or lesion in area difficult to access but seen on ultrasound, MRI | Surgical (open) biopsy may be incisional (to remove tissue samples for testing) or excisional (to remove the entire mass, as in a lumpectomy). This procedure is less used because the ultrasound-guided biopsy, MRI-guided biopsy, and stereotactic biopsy are attempted prior to deciding on surgical biopsy. | Breast or general surgeon surgically removes the mass or suspicious area of the breast. This involves giving you sedation or general anesthesia (that is, being "put to sleep"). |
| Used for abnormal lesion(s) visualized only on tomosynthesis mammography | Tomosynthesis-guided biopsy (the machine is upright and is often added to existing equipment such as machine for stereotactic biopsy). | The breast that is being biopsied will be compressed (similar to a mammogram), while tomo mammographic technique is used to locate the abnormality. The radiologist injects a local anesthetic such as Lidocaine into the skin and deeper tissues to numb the area. A very small skin incision is made. The abnormality will be located by tomo, and several tissue samples will be extracted and sent to the pathologist for interpretation. |
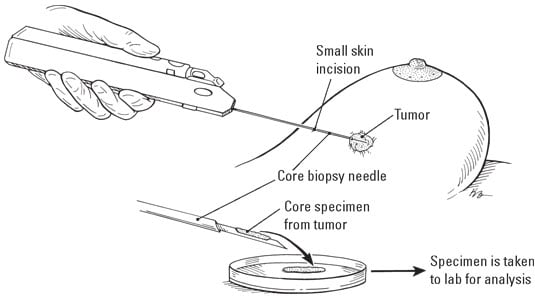 Illustration by Kathryn Born
Illustration by Kathryn BornCore biopsy.
If your doctor ordered a stereotactic or MRI-guided core needle biopsy, the procedure may strike you as a little odd. With a stereotactic biopsy, you lie face down on a table with your soon-to-be-biopsied breast extending down through a hole in the table. Your breast is squeezed between two mammogram plates, and X-rays are taken to show the doctor where to poke the needle.
The MRI-guided core needle biopsy is similar, but your breasts nestle in a depression in the table. Although it sounds like something out of the Middle Ages, your doctor is performing a modern medical procedure.