No further tests are technically required to make a multiple sclerosis (MS) diagnosis when a patient’s medical history and neurologic exam provide evidence of two episodes of demyelination that are separated in time and space.
However, because no one diagnostic test is conclusive, various screenings and exams, along with magnetic resonance imaging (MRI) scanning, are typically used to confirm the initial diagnosis or to help the neurologist identify a second episode of demyelination (if it wasn’t apparent from the history or exam). These other tests can also help to rule out other diseases that could be masquerading as MS.
Evoked potential testing to confirm MS
Evoked potential (EP) tests are recordings of the central nervous system’s electrical response to the stimulation of specific nerve pathways (visual, auditory, and sensory) that are commonly affected in MS.
These electrical responses are recorded from brain waves by using electrodes taped to your head. Because demyelination results in a slowing of response time, EPs can sometimes provide evidence of demyelination along nerve pathways that isn’t otherwise apparent to the neurologist from the medical history or neurologic exam.
For example, if Susie goes to her neurologist with one symptom that’s characteristic of MS, such as numbness and tingling or extreme fatigue, and she reports an episode of blurred vision a few years ago, the neurologist may request visual evoked potential (VEP) testing to find out whether the blurred vision was caused by an episode of demyelination of the optic nerve, called optic neuritis.
Of the three types of EP tests that neurologists use (visual, auditory, and sensory), the VEP test is generally considered the most useful in diagnosing MS because 80 percent of people with the disease have slowed responses on this test.
So, if Susie’s VEP is abnormal, her neurologist has evidence of two separate areas of demyelination, helping to confirm the MS diagnosis. But, if Susie’s VEP is normal, the doctor needs to continue looking for additional evidence of demyelination.
When you’re undergoing an EP test, a technician applies gel (to promote electrical conduction) and electrodes to your head and body at certain locations that are determined by the type of response being recorded. For example, when visual-evoked responses are recorded, the electrodes are placed at the back of your scalp over the brain areas that register visual stimuli. For other EP tests, the electrodes are placed at different points on the head and body.
Different stimuli are delivered for each test. For example, a strobe light or screen with a checkerboard pattern is flashed for the visual test; clicking noises or a tone are delivered through headphones for the auditory test; and a mild electrical pulse is delivered at the wrist or knee for the general sensory test.
The procedure, which takes approximately 45 minutes per test, is non-invasive and completely painless except for the slight (and we mean slight) discomfort caused by the mild shock given for the sensory evoked potential test.
Lumbar puncture to confirm MS
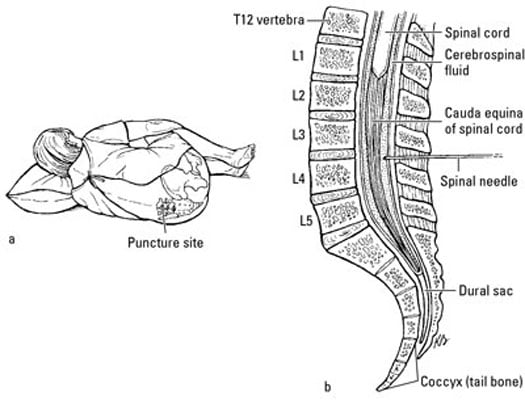
The lumbar puncture or LP (also known as the spinal tap) allows your neurologist to examine the cerebrospinal fluid (CSF) that cushions and protects your brain and spinal cord. The doctor obtains the CSF by inserting a spinal needle into your lower spine, as shown here:
The CSF is then analyzed for evidence of an abnormal immune response in the CNS. Specifically, the neurologist is looking for increased production of certain immune proteins (IgG). Using a method called protein electrophoresis, some of this IgG may show up as stripes or bands (called oligoclonal bands). Nearly 90 percent of patients with MS have these bands, making them an important piece of evidence in the diagnostic process.
Because other conditions can also produce oligoclonal bands and because 10 to 21 percent of people with MS can actually have normal cerebrospinal fluid findings, the LP by itself can’t make the diagnosis. However, the findings can help the neurologist build the case for an MS diagnosis or exclude it.
The LP, which generally isn’t high on anyone’s list of fun things to do, can be performed in about 20 minutes in your neurologist’s office. The doctor injects a local anesthetic into your back. He or she then inserts a spinal needle into the fluid-filled space that surrounds the nerves below the bottom end of your spinal cord, withdraws a small amount of CSF (we promise that it’s really not as awful as it sounds), and then asks you to straighten your legs. Immediately after removing the needle, the doctor applies pressure to the puncture site and asks you to lie still for about 30 to 45 minutes. This waiting period helps reduce the risk of severe headache caused by the internal leakage of CSF, which occurs following approximately 20 percent of LP procedures. The doctor also recommends rest and plenty of fluids after the LP.
Blood tests to rule out non-MS problems
Even though no definite blood tests exist for MS, blood tests can positively rule out other causes for neurologic symptoms, such as Lyme disease, collagen-vascular diseases, certain hereditary disorders, and HIV/AIDS.